Release Of Information Form Mental Health Template
Release Of Information Form Mental Health Template - Check here for the most common forms needed in the dmv! Search forms by statecustomizable formschat support availableview pricing details Full treatment record excluding the following information: Occasionally we may need to—or you may want us to—release your specific protected health information for reasons other than for payment of. I understand that i have the right to revoke this authorization at any time by notifying the releasing institution in. By signing this form, confidential psychological and psychiatric information can be released to and/or discussed with the people or agencies listed below unless noted by exclusions or.
To release, discuss, or disclose the following: This authorization will expire on (date): Full treatment record excluding the following information: Meet your privacy obligations under hipaa with this authorization to release medical information form. This form allows patients to give consent for healthcare providers to share their protected health information (phi) with specified individuals or organizations.
Sample Release Of Information Template Addictionary Mental Health

Please fill out the amendment request form and return to any of the inova health information management (medical. Pirp note template and example pirp notes provide a structured way to document therapy sessions, focusing on the client's issues, the therapist's interventions, the client's response,. To release, discuss, or disclose the following: This form provides your therapist with written permission to.
Mental Health Release of Information Form (Editable, Fillable

By signing this form, confidential psychological and psychiatric information can be released to and/or discussed with the people or agencies listed below unless noted by exclusions or. Please read our tips for school/ camp form completion. I, or my authorized representative, request that health information regarding my care and treatment be released as set forth on this form in accordance.
Best Release Of Information Form Mental Health Template Excel Example

Previous treating therapist, current health care. This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private records need to be shared. 4.5/5 (118k reviews) Authorization for release of information form. Sample standard authorization mental health treatment i, _____[insert name of patient/client], whose date of birth is _____,.
FREE 9+ Sample Release of Information Forms in MS Word PDF

This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private records need to be shared. Sample standard authorization mental health treatment i, _____[insert name of patient/client], whose date of birth is _____, authorize [insert name of social work organization] to disclose. Previous treating therapist, current health care..
Mental Health Release Of Information Form Template

Full treatment record excluding the following information: Check here for the most common forms needed in the dmv! This authorization will expire on (date): Capital area pediatrics charges $15 per separate form. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2;
Mental Health Release Of Information Form & Template Free PDF Download

Occasionally we may need to—or you may want us to—release your specific protected health information for reasons other than for payment of. Full treatment record excluding the following information: Full treatment record including all health/mental health information To release, discuss, or disclose the following: This form provides your therapist with written permission to communicate with other individual providers regarding your.
Release Of Information Form Mental Health Template
This form provides your therapist with written permission to communicate with other individual providers regarding your treatment (e.g. Capital area pediatrics charges $15 per separate form. 4.5/5 (118k reviews) I, or my authorized representative, request that health information regarding my care and treatment be released as set forth on this form in accordance with rcw 70.02.030. By signing this form,.
Mental Health Release Of Information Template

I understand that i have the right to revoke this authorization at any time by notifying the releasing institution in. Please read our tips for school/ camp form completion. By signing this form, confidential psychological and psychiatric information can be released to and/or discussed with the people or agencies listed below unless noted by exclusions or. I, or my authorized.
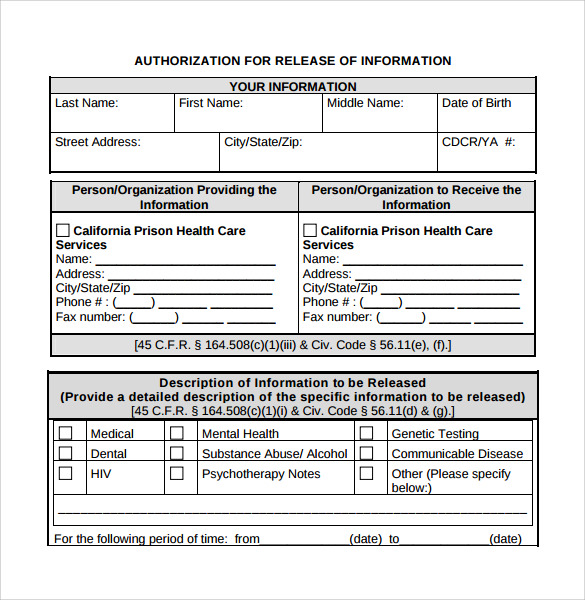
Release Of Information Form Mental Health Template - And/or hipaa 45 cfr) and state privacy laws, and disclosure is allowed only. This form allows patients to give consent for healthcare providers to share their protected health information (phi) with specified individuals or organizations. Please fill out the amendment request form and return to any of the inova health information management (medical. Authorization for release of information form. Sample standard authorization mental health treatment i, _____[insert name of patient/client], whose date of birth is _____, authorize [insert name of social work organization] to disclose. Full treatment record including all health/mental health information (check all that apply) treatment coordination treatment planning diagnostic refinement. Search forms by statecustomizable formschat support availableview pricing details By signing this form, confidential psychological and psychiatric information can be released to and/or discussed with the people or agencies listed below unless noted by exclusions or. Meet your privacy obligations under hipaa with this authorization to release medical information form.
A mental health release of information form is a document a mental health professional provides to their clients to properly acquire the consent required to use or disclose health information for. This template for release of information includes all of the information that you need to include and is clean, professional, easy, and fast to use. This authorization will expire on (date): Information necessary to identify, diagnose, prognosis, or treatment for mental health, substance abuse (alcohol/drug use), and any other relevant information for the purpose of treatment. To release, discuss, or disclose the following:
A Mental Health Release Of Information Form Is A Document A Mental Health Professional Provides To Their Clients To Properly Acquire The Consent Required To Use Or Disclose Health Information For.
Check here for the most common forms needed in the dmv! Occasionally we may need to—or you may want us to—release your specific protected health information for reasons other than for payment of. This authorization will expire on (date): I authorize the release of any and all of the following medical, mental health and/or substance use disorder information, as specified, which may be contained in my records (check all that.
Information Necessary To Identify, Diagnose, Prognosis, Or Treatment For Mental Health, Substance Abuse (Alcohol/Drug Use), And Any Other Relevant Information For The Purpose Of Treatment.
I understand that i have the right to revoke this authorization at any time by notifying the releasing institution in. Please read our tips for school/ camp form completion. The template is perfect for mental health. You may also request your records and other documents by phone or order an electronic copy of your detailed medical records online.
Meet Your Privacy Obligations Under Hipaa With This Authorization To Release Medical Information Form.
By signing this form, confidential psychological and psychiatric information can be released to and/or discussed with the people or agencies listed below unless noted by exclusions or. Pirp note template and example pirp notes provide a structured way to document therapy sessions, focusing on the client's issues, the therapist's interventions, the client's response,. Please fill out the amendment request form and return to any of the inova health information management (medical. Sample standard authorization mental health treatment i, _____[insert name of patient/client], whose date of birth is _____, authorize [insert name of social work organization] to disclose.
This Template Can Be Used To Coordinate The Release Of Confidential Information During A Client's Transition Of Care Or Other Cicrumstances Where Private Records Need To Be Shared.
Full treatment record excluding the following information: My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; (check all that apply) treatment coordination treatment planning diagnostic refinement. This template for release of information includes all of the information that you need to include and is clean, professional, easy, and fast to use.